
Medicine, genocide and crimes against humanity. Medicina, genocidio y crímenes de lesa humanidad. ENG ESP

Accountability for human rights. Rendición de cuentas y derechos humanos
ENGLISH
Opinion. British Medical Journal
Medicine’s reckoning with genocide and crimes against humanity
30 October 2025
Rubin Minhas, managing partner1, Duha Shellah, chair2, Nick Maynard, professor of surgery3, Guy Goodwin-Gill, emeritus professor of international refugee law4, Iain Chalmers, cofounder5, Gene Feder, professor of primary health care6
Accountability for human rights must guide every collaboration in medicine and science
From Darfur to Tigray to Myanmar, attacks on healthcare have become a weapon of war. The destruction of hospitals and killing of healthcare workers in Gaza has been an integral part of what a United Nations (UN) inquiry has deemed to be genocide in Gaza.12
Genocide, together with the 11 crimes against humanity (including torture, rape, forcible transfer, persecution, and apartheid) and war crimes, are collectively known as atrocity crimes.3 The prohibition of genocide is an absolute rule (jus cogens) of international law—so fundamental that no government can ignore or override it. Every state is bound to prevent, stop, and punish those responsible. Early warnings often come from civil society and journalists, then non-governmental organisations such as Human Rights Watch and Amnesty International.45 Formal early warning systems can predict atrocities up to a year before mass killing begins.6
Atrocities are recurrent, exposing a systemic failure of prevention. As in public health, the precautionary principle demands action amid uncertainty. For medicine, that means disengaging from institutions implicated in genocide—refusing collaborations that sustain impunity. Acting early is both a humanitarian and professional duty—the antidote to paralysis as the world grows desensitised to violence.7
History shows that what medicine once defended as neutrality under slavery, apartheid, and Nazism was later condemned as complicity. The same tension now faces academia. Responses to Israeli human rights abuses in the Occupied Territories have been largely grassroots, coalescing through professional networks and campaign alliances. In 2015, more than 300 UK academics pledged non-cooperation under the Palestinian Campaign for the Academic and Cultural Boycott of Israel,89 yet a decade later no UK university has severed ties. Partnerships such as the Britain-Israel Research and Academic Exchange Partnership link UK universities and medical charities1011 to Israeli institutions with reported involvement in defence related research, including drones and missile technology.121314
After Russia’s invasion of Ukraine, UK Research and Innovation suspended grants and universities severed partnerships—treating boycott as a moral imperative.15 Such double standards expose the absence of guiding principles and risk complicity with governments and institutions either failing to prevent, or actively engaged in, atrocities. What is needed is a transparent process for justifying ethical disengagement when the risk of atrocity arises—balancing preventive action with important values such as academic freedom and scientific universalism.
Atrocity makes universality impossible by destroying the equal moral position on which it depends. The philosopher John Rawls captured this ideal through his veil of ignorance: decisions are fair only when made as if one could be anyone, ensuring that every life holds equal worth.16 Genocide and crimes against humanity negate that premise, deciding in advance whose lives do not count. In such conditions, neutrality must be active—maintaining equal moral distance to uphold the rights of all peoples. When medicine or academia continue collaboration instead, academic freedom becomes privilege, scientific universalism becomes partiality, and silence becomes complicity.
Concerns that individual clinicians might be disadvantaged by academic disengagement are misplaced; existing guidance17 and scholar-at-risk schemes18 protect individuals while suspending ties with institutions formally implicated in atrocity. Disengagement from institutions implicated in genocide remains the only means of restoring moral equipoise.
Disengagement interventions like sanctions and consumer boycotts can wield both economic and moral force; their power lies in moving markets and conscience. But in health and academia, the purpose is ethical disengagement to avoid complicity.
The Nestlé boycott,23 the rejection of tobacco sponsorship,24 and academic boycotts of Israeli institutions by the Middle East Studies Association25 and the American Anthropological Association26 share that intent: refusal to collude with harm.
Ethical double standards corrode our principles: the Modern Slavery Act demands corporate transparency,27 yet no duty requires scrutiny of collaborations with institutions implicated in atrocity.
Medicine already follows non-statutory standards—ethics committees, conflict of interest declarations, and frameworks such as CONSORT and PRISMA—that carry moral force without legal mandate. Aligning medical ethics with jus cogens norms would close the gap between legality and morality, holding medicine to the same universal standards that govern humanity. One question, examining the human cost, should guide us: does a collaboration risk complicity in genocide or crimes against humanity?
Ethical engagement should begin with human rights statements that disclose links to institutions or states implicated in atrocity across all research, grants, ethics reviews, and publications. Institutions can embed such due diligence—as Erasmus University has done by reviewing partners, their military ties, and human rights records—so accountability crosses borders.17
Real time field reports from non-governmental organisations offer more practical evidence for prevention than probabilistic early warning models28 or retrospective rulings by the International Court of Justice.
Clear signals should guide judgment: gravity—the scale of the crimes; necessity—when disengagement is among the few levers left; effectiveness—whether disengagement shifts incentives or reduces harm; universality—whether inconsistent responses imply some lives count for less; and entanglement—when collaboration creates moral or material ties or offers reputational cover.
Nearly eight decades after the Genocide Convention in 1948,29 prevention has advanced in principle but faltered in practice. Many states remain indifferent, but medicine must not.30
Beginning with genocide, medical and academic leaders have a duty to implement reforms to safeguard the line between valuable collaboration and toxic complicity, break institutional silence, and declare medicine’s commitment to the right to existence and life for all peoples, in all states.
Footnotes
Competing interests: The authors declare they have no conflicts of interest.
ESPAÑOL

Fergie Chambers facing US extradition from Spain. Fergie Chambers, detenido en Ibiza para extraditarlo a Estados Unidos. ENG ESP
The use of counterterrorism powers to target left-wing activists and political movements. Uso de legislación contraterrorista para lesionar actividades propalestina.
Publicado hace 2 días.
Ética médica. Están torturando hasta matar a nuestro compañero Abu Safiya. ¿Qué vas a hacer?
¿Vas a permanecer en silencio e impasible?
Publicado hace 5 días.
España. Evacuaciones sanitarias sanitarias infantiles. No hay motivo para el orgullo, señora ministra
Le pedimos un esfuerzo mayor para evacuar a más pacientes palestinos.
Publicado hace 10 días.
Dr Abu Safiya. "Esta es la última vez que me ves". "This is the last time you'll see me" ESP ENG
Physicians for Human Rights Israel, (PHRI): riesgo «inminente» para la vida del doctor Hussam Abu Safiya. Physicians for Human Rights Israel of an "imminent" risk to the life of Dr. Hussam Abu Safiya
Publicado hace 12 días.
Israel. The physician: “I didn’t come to treat you. I came to torture you.” El médico: «No vine a curarte. Vine a torturarte».
Tortures unrelated to interrogations or intelligence gathering. Torturas no relacionadas con interrogatorios ni con la recopilación de información
Publicado el 30 de junio.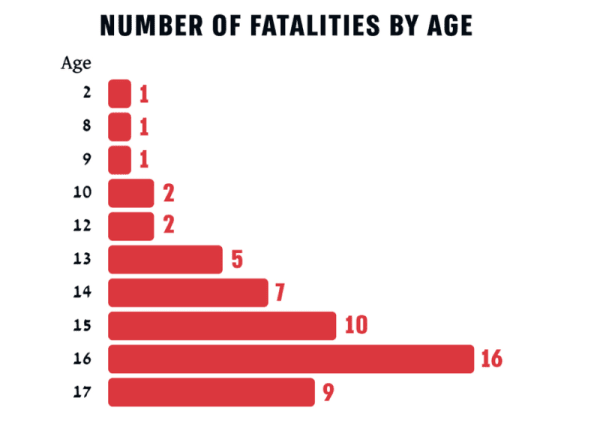
Unshielded Childhood: 54 Palestinian children and teenagers killed by Israel in the West Bank in 2025. Infancia inerme. 54 niños-adolescentes asesinados en 2025 en Cisjordania. ENG ESP
As of 6 June 2026, Israel was still holding 18 of the 54 bodies. A 6 de junio de 2026, Israel mantiene secuestrados 18 de los 54 cuerpos.
Publicado el 29 de junio.
British Medical Association votes down IHRA anti-semitism definition. La Asociación Médica Británica rechaza la definición de antisemitismo de la IHRA. ENG ESP
To protect doctors criticizing Israel from NHS discipline. Para proteger a los médicos que critican a Israel de posibles sanciones en el Servicio Nacional de Salud.
Publicado el 28 de junio.
The Israeli Medical Association (IMA) is acting like the Israel Defense Forces (IDF)'s mouthpiece. La Asociación Médica Israelí (AMI) actúa como portavoz de las Fuerzas de Defensa de Israel (FDI). ENG ESP
"How can we, doctors, stand aside?". "¿Cómo podemos nosotros, los médicos, quedarnos al margen?"
Publicado el 27 de junio.Ver más / See more
