
Boicot Austedo (Teva). Boycott Austedo (Teva). ENG ESP
Huntington disease. Tardive dyskinesia. Discinesia tardía. Enfermedad de Huntington
ENGLISH
Introduction
ESPAÑOL
Introducción
Austedo (deutetrabenazine) está comercializado en Australia, China y Estados Unidos, y en proceso de aprobación en la Unión Europea, para el tratamiento de la corea de Huntignton y de la discinesia tardía.
Se dispone de tres fármacos para el tratamiento de la discinesia tardía: tetrabenazina (brand name: Xenazine, hay genéricos varios), valbenazina (Ingrezza) y deutetrabenazina (Austedo).
En Estados Unidos, para hacer boicot a Teva se puede emplear valbenazine (Ingrezza) con mejores resultados que deutetrabenazine (Austedo). También, off label, tetrabenazina (brand name: Xenazine, hay genéricos varios).
En general, el mejor boicot a Teva, que ahorra sufrimientos inmensos, es el uso racional de los neurolépticos (antipsicóticos) y así evitar el efecto adverso de la discinesia tardía.
Por cierto, Teva comercializa Uzed, risperidona (con un mecanismo "Steady Teq Technology” para su liberación lenta) y en 2026 comercializará olanzapina con el mismo mecanismo. Ambos neurolépticos producen discinesia tardía.
Boicot a Austedo, un medicamento de Teva para los movimientos involuntarios
Health Workers for Palestine, Spain HW4PS, 30 noviembre 2025
https://hw4p.es/ hcw4palestinespain@gmail.com
Corea
El término corea alude a “danza” (“choreia”, en griego).
La corea es un trastorno neurológico que se caracteriza por movimientos corporales involuntarios e impredecibles.
Se producen espasmos, tic y tirones musculares que suelen localizarse en las partes distales de los miembros, especialmente en las manos, y también en la cara.
La gravedad de la corea puede variar desde movimientos leves y apenas perceptibles hasta síntomas graves y debilitantes que interfieren con las actividades diarias, como hablar y deglutir.
Aunque existen muchas causas de corea, las más importantes son la enfermedad de Huntington, fiebre reumática, la corea inducida por tratamiento prolongado con fármacos (“discinesia tardía”, especialmente neurolépticos, empleados para el tratamiento de enfermedades mentales como esquizofrenia, trastorno bipolar, etc), trastornos metabólicos (como hipertiroidismo e hipoparatiroidismo), enfermedades autoinmunes (por ejemplo, lupus eritematoso, etc), etc.
Enfermedad de Huntington
La enfermedad de Huntington es una grave y rara enfermedad neurológica, hereditaria y degenerativa que afecta a la coordinación motora, el ánimo y la memoria.
Se debe a una mutación genética en el cromosoma 4 y tiene un pronóstico de 15-20 años de media de supervivencia tras el comienzo de los síntomas (que suelen aparecer entre los 30 y 50 años de edad), con un cuadro progresivo de movimientos anormales e involuntarios de tipo coreico que afectan con mayor frecuencia a los miembros inferiores y a la cara (muecas repentinas), haciéndose cada vez más difícil el habla y la deglución.
Es enfermedad genética autosómica dominante (desencadena la enfermedad la presencia de una sola copia del gen mutado, del padre o de la madre).
Su prevalencia es baja, de 5 casos por cada 100.000 habitantes (1). Es decir, unas 23.000 pacientes en la Unión Europea y unos 17.000 en Estados Unidos.
Discinesia tardía
La discinesia tardía es un trastorno neurológico generalmente irreversible, caracterizado por movimientos involuntarios repetitivos en la región orofacial que también puede afectar extremidades y tronco.
La discinesia tardía se produce como efecto adverso del empleo prolongado (de ahí lo de “tardía”) de neurolépticos, medicamentos para el tratamiento de enfermedades mentales como esquizofrenia, psicosis recurrente y trastorno bipolar, y en otras muchas situaciones como demencia, agitación, depresión, síndrome de Tourette, trastornos conductuales en infancia, cuadro de delirio, etc.
La discinesia tardía es también efecto adverso de levodopa (medicamento para la enfermedad de Parkinson), metoclopamida (empleada para vómitos, naúseas y vértigo), etc.
Se da en un 20% de los pacientes tratados crónicamente, siendo más frecuente en mujeres y en la ancianidad.
Prevalencia de la discinesia tardía
La prevalencia de la discinesia tardía va paralela a la del uso de neurolépticos, que es creciente. Es decir, la discinesia tardía es enfermedad de causa “médica”, creada por el cada vez más frecuente tratamiento crónico con medicamentos neurolépticos.
Según Heather DeMyers, vicepresidente de US Innovative Medicines Marketing, de Teva, en Estados Unidos puede haber casi 800.000 personas con discinesia tardía, pero sólo el 15% está diagnosticado y sólo el 5% tratado (2). Si fuera cierto, en la Unión Europea habría casi 1.000.000 de pacientes con discinesia tardía.
Quizá estas cifras formen parte de la estrategia de Teva de utilizar medios innovadores y tácticas sociales para incrementar el reconocimiento de marca y apoyar la concienciación sobre la enfermedad (disease-awareness) (3).
En todo caso, es innegable el creciente número de pacientes que sufren discinesia tardía, ligado al efecto adverso del uso prolongado de los neurolépticos en sus aplicaciones recomendadas, y en otras muchas más. Por ello, incluso es producto comercial el análisis del “mercado” en aumento creado por la discinesia tardía (4).
La discinesia tardía lleva a la típica cascadaiv de uso de un medicamento que conlleva el empleo de otro medicamento para paliar los efectos adversos del primero.
Tratamiento de la discinesia tardía (y otras coreas)
Lo clave es disminuir en duración y cantidad el uso de neurolépticos, para prevenir el efecto adverso. Pero el actual enfoque biológico de la Psiquiatría lleva a lo contrario, al incremento de la prevalencia de su prescripción.
Se dispone de tres fármacos para el tratamiento de la discinesia tardía: tetrabenazina (En EEUU, Xenazine, hay genéricos varios, y en España Nitoman, y dos genéricos), valbenazina (Ingrezza) y deutetrabenazina (Austedo).
Son medicamentos inhibidores del transportador vesicular de monoaminas 2 (VMAT2) (6). VMAT2 es una proteína que reduce la cantidad de neurotransmisores en las células nerviosas. La inhibición de VMAT2 conduce a un agotamiento de la dopamina presináptica y reduce la cantidad de dopamina liberada en la sinapsis (7). Ingrezza se metaboliza y actua selectivamente con mayor afinidad sobre VMAT2vi. Se cree que esto ayuda a controlar los movimientos corporales involuntarios pero se desconoce el mecanismo final de acciónvii.
En España sólo está comercializada la tetrabenazina (Nitoman, y genéricos, en Estados Unidos Xenazine, hay genéricos varios) para el tratamiento de la enfermedad de Huntington y no tiene indicación en ficha técnica para discinesia tardía (su uso es off-label). Su peor efecto adverso es akatisia (sensación incontrolable de inquietud y necesidad constante de moverse que afecta al bienestar físico y mental).
Valbenazina (Ingrezza) y deutetrabenazina (Austedo) sí tienen indicación en discinesia tardía, pero no están comercializadas en la Unión Europea. Austedo está en proceso de aprobación (9). No es un medicamento nuevo, como señala la Agencia Europea del Medicamento, sino el mismo Nitoman con un hidrógeno (deuterio) añadido, con el propósito de prolongar su vida media (10).
La discinesia tardía leve no suele recibir tratamiento específico, salvo monitorizar la evolución de los síntomas y valorar la posibilidad de reducir la dosis del neuroléptico. En el caso de la discinesia tardía grave, se debe valorar disminuir la dosis del mismo, o sustituirlo por otro, a ser posible clozapina. En casos concretos, los síntomas discinéticos pueden mejorar con las benzodiacepinas, como clonazepam, o se puede emplear tetrabenazina.
Efectos adversos de tetrabenazina (en España Nitoman, y dos genéricos, en Estados Unidos Xenazine, hay genéricos varios), valbenazina (Ingrezza) y deutetrabenazina (Austedo)
Los efectos secundarios más comunes de Nitoman (10 % o más de los pacientes): sedación (somnolencia o somnolencia extrema), fatiga, dificultad para dormir, depresión y akatisia.
Austedo también puede provocar efectos secundarios graves como trastornos del ritmo cardíaco (prolongación del intervalo QT del electrocardiograma que puede desencadenar una arritmia denominada torsión de puntas que se manifiesta como síncope, mareos o palpitaciones y suele resolverse espontáneamente, si bien en ocasiones puede originar una fibrilación ventricular y causar la muerte), akatisia, temblores, rigidez muscular; problemas de equilibrio o coordinación; o reacción grave del sistema nervioso: rigidez muscular, fiebre alta, sudoración, confusión, cambio del ritmo cardíaco.
Los efectos secundarios comunes de Austedo: somnolencia; cansancio; boca seca; secreción o congestión nasal, dolor de garganta; problemas para dormir y diarrea.
Ingreza puede causar efectos secundarios graves que incluyen: problemas del ritmo cardíaco (prolongación del intervalo QT del electrocardiograma que puede desencadenar una arritmia denominada torsión de puntas que se manifiesta como síncope, mareos o palpitaciones y suele resolverse espontáneamente, si bien en ocasiones puede originar una fibrilación ventricular y causar la muerte) y parkinsonismo (temblores, rigidez corporal, dificultad para moverse o caminar, o para mantener el equilibrio).
El efecto secundario más común de la valbenazina es la somnolencia, también problemas de equilibrio, dolor de cabeza, inquietud, boca seca, estreñimiento, visión borrosa.
Estos tres medicamentos deben evitarse en pacientes con antecedentes de ideas y comportamientos suicidas, con depresión grave o con depresión mal controlada. También en pacientes que tomen inhibidores potentes de la enzima CYP2D6 (paroxetina, fluoxetina, quinidina, etc), beban alcohol o tomen otros medicamentos sedantes.
Campaña de Teva para introducir Austedo
Austedo no es más que el Nitoman/Xenazine, desarrollado en los 60 del siglo XX, modificado, pero es el producto estrella de Teva del que prevé ingresos de más de 1.200 millones de dólares en 2025 (sin estar autorizado en la Unión Europea) (11). Su estrategia de ventas se centra en el tratamiento de la discinesia tardía.
Para ello busca incrementar el “mercado” y produce anuncios con personajes famosos, promociona páginas de propaganda disimulada y realiza estudios “científicos” que, al “alertar” de la enfermedad, incrementan el diagnóstico y llevan al tratamiento.
Se puede encontrar actividad de concienciación sobre la enfermedad (disease-awareness) para profesionales (12), pacientes (13) y público en general (14). También publicaciones “científicas” múltiples para incrementar la alarma sobre la discinesia tardía, siempre firmadas por autores con conflictos de interés por su relación con Teva (vea la NOTA al final).
En un próximo futuro es de esperar la redacción de “consensos” acerca de la discinesia tardía ampliando los criterios diagnósticos, separando el diagnóstico de la experiencia vital (“biometría”) y adelantando el tratamiento, en relación con la financiación por Teva de sociedades de neurología y psiquiatría. Por lo mismo se incrementarán las reuniones, cursos y mesas en congresos sobre dicha cuestión para profesionales de la sanidad y pacientes-familiares.
Austedo versus Ingrezza
En Estados Unidos, el costo de 60 tabletas de Austedo de 12 mg es de alrededor de $7.465, y se toman 2 o 3 al día, según la respuesta. El costo de 60 tabletas de 12 mg de Austedo XR (de liberación prolongada) es de $7,465 y se toman 1 o 2 al día, según la respuesta. Esto equivale un costo anual de unos $80-90.000 por año de tratamiento.
En Estados Unidos, Ingrezza (valbenazina) cuesta aproximadamente $6.252 por treinta cápsulas de 40 mg y $7.038 por treinta cápsulas de 80 mg, y se toman 80 mg al día. Esto equivale a un costo anual de unos $70-80.000 por año de tratamiento.
En Estados Unidos, tetrabenazine (allí Xenazine) cuesta unos $400 al mes; es decir, un coste de unos $4-5.000 al año.
En España, hay 3 medicamentos con tetrabenazina 25mg, con 112 comprimidos de precio de 123,54€: el de marca, Nitoman, y los genéricos que los producen Aristo y Sun. Se toman 3 comprimidos al día lo que equivale a un costo anual de unos 1.200€.
Según un estudio cuyos autores tienen conflictos de interés con Neurocrine Biosciences (que produce Ingrezza), en el tratamiento de la discinesia tardía, los pacientes tratados con Ingrezza tuvieron mejor respuesta al tratamiento al año, vivieron más tiempo y acumularon más AVAC (años de vida ajustados por calidad) que los pacientes que recibieron Austedo (15).
Utilizando el criterio de respuesta AIMS (Abnormal Involuntary Movement Scale), la razón costo-efectividad incremental fue de $9,951/AVAC para Ingrezza en comparación con Austedo. En comparación, los pacientes tratados con Ingrezza acumularon más AVAC e incurrieron en menores costos a lo largo de la vida ($252,311 frente a $283,208) que los pacientes tratados con Austedo.
En otro estudio, Ingrezza tuvo también ventajas, por ejemplo por la forma de administración en pacientes con dificultades para deglutir (16).
Boicot a Austedo
En la Unión Europea, por ahora, el único tratamiento específico de la discinesia tardía es tetrabenazina (Nitoman en España y sus genéricos) empleada off-label pues según su ficha técnica sólo está autorizado para tratar la corea de Huntington.
En el próximo futuro se aprobará en la Unión Europea la comercialización de deutetrabenazina (Austedo) tanto para la discinesia tardía como para la corea de Huntington.
Por ahora no se prevé la comercialización de valbenazina (Ingrezza), que obtiene mejores resultados que deutetrabenazina (Austedo).
El boicot a Austedo se plantea, pues, en el seguimiento de los movimientos de asociaciones y sociedades científicas de neurología y psiquiatría (y de pacientes) para evitar la ampliación de la definición de discinesia tardía y para disminuir el uso de los medicamentos que la producen.
Además, conviene tener presente que los neurolépticos en las psicosis, como esquizofrenia, pueden producir más daños que beneficios (17) (18), que se puede evitar su uso prolongado, o al menos disminuir la dosis (19) y que las perspectivas a largo plazo son mejores cuanto menos se utilicen (un primer año de tratamiento con antipsicóticos, incluso en dosis moderadas, probablemente induce cambios iatrogénicos en el cerebro que persisten y tienen un impacto a largo plazo) (20). Respecto al uso de neurolépticos en la demencia senil, desde 2004 se viene alertando del particular riesgo de seguridad de los antipsicóticos en personas mayores (riesgo cerebrovascular, neumonías, caídas, muerte…). En particular preocupa la incidencia de casos de ictus y mortalidad en personas con demencia (21).
Irónicamente, Teva también comercializa un neuroléptico, Uzed, risperidona (con un mecanismo "Steady Teq Technology” para su liberación lenta) y en 2026 comercializará olanzapina con el mismo mecanismo. Es decir, Teva hace negocio con neurolépticos y con el efecto adverso de los mismos, la discinesia tardía.
NOTA
Teva desarrolla una frenética “línea científica” con publicaciones en revistas médicas, generalmente a través de “key opinion leaders” (líderes de opinión) ligados a la empresa.
Algunos ejemplos:
- La discinesia tardía no diagnosticada ni tratada dificulta el cumplimiento del tratamiento con antipsicóticos Dr. Daniel Kremens.
https://espanol.medscape.com/verarticulo/5913032?form=fpf
-Conflictos de interés: El Dr. Daniel Kremens ha declarado los siguientes conflictos de interés económico pertinentes: Se desempeña o se ha desempeñado como consultor para: Teva Pharmaceuticals; Amneal; Acadia; Supernus; Adamas; AbbVie; Merz; Allergan; Acorda; Kyowa Kirin; Neurocrine; Bial; Cerevel Se desempeña o se ha desempeñado como conferenciante o miembro de un gabinete de conferenciantes para: Teva Pharmaceuticals; Amneal; Acadia; Supernus; Adamas; Acorda; Kyowa Kirin; Neurocrine.
-Re: Ganz ML, Chavan A, Dhanda R, et al. Cost-effectiveness of valbenazine compared with deutetrabenazine for the treatment of tardive dyskinesia. J Med Econ. 2021;24(1):103–113. https://www.tandfonline.com/doi/full/10.1080/13696998.2021.1948230
-Conflictos de interés: SL y RR son empleados de Teva Pharmaceuticals y poseen acciones y opciones sobre ellas. WX, ZZ y RA son empleados de Analysis Group, Inc., que ha recibido honorarios de consultoría de Teva Pharmaceuticals.
-Clinical practice guidelines for the treatment of tardive dyskinesia in Europe: A descriptive review
https://pubmed.ncbi.nlm.nih.gov/40671306/
-Conflictos de interés: Mark J. Edwards ha formado parte de consejos asesores de Teva Pharmaceuticals y ha recibido honorarios por eventos educativos en nombre de Teva Pharmaceuticals. Pierre Michel Llorca ha sido consultor de Teva Pharmaceuticals y miembro de Consejos de Monitoreo de Seguridad de Datos o consejos asesores de Teva Pharmaceuticals, y ha recibido honorarios por eventos educativos en nombre de Teva Pharmaceuticals. Maurice T. Driessen, Krzysztof Duma y Nayla Chaijale son empleados y accionistas de Teva Pharmaceuticals. Liza Sopina ha recibido pagos de Yorker Health. Sameer Kotak es empleado de Yorker Health y ha recibido pagos de Teva Pharmaceuticals en relación con este estudio. Andrea Fagiolini es o ha sido consultor y/o ponente y/o ha recibido becas de investigación de Angelini Pharma, Boehringer Ingelheim, Idorsia Pharmaceuticals, Italfarmaco SpA, Lundbeck, Janssen Pharmaceuticals, Medicamenta, Mylan, Otsuka Pharmaceutical, Pfizer, Recordati, Rovi, Sunovion, Teva Pharmaceuticals y Viatris. David Taylor ha recibido honorarios personales de Lundbeck, Otsuka y Janssen; se desempeñó como consultor para Viatris y Teva Pharmaceuticals; y posee acciones en 428 Pharma, Myogenes y Saladax. Christoph Correll ha sido consultor o asesor, o ha recibido honorarios, de AbbVie, Acadia, Adock Ingram, Alkermes, Allergan, Angelini, Aristo, Biogen, Boehringer-Ingelheim, Bristol Myers Squibb, Cardio Diagnostics, Cerevel, CNX Therapeutics, Compass Pathways, Darnitsa, Delpor, Denovo, Eli Lilly, Gedeon Richter, Hikma, Holmusk, IntraCellular Therapies, Jamjoom Pharma, Janssen/J&J, Karuna, LB Pharma, Lundbeck, MedInCell, MedLink, Merck, Mindpax, Mitsubishi Tanabe Pharma, Maplight, Mylan, Neumora Therapeutics, Neurocrine, Neurelis, Newron, Noven, Novo Nordisk, Otsuka, PPD Biotech, Recordati, Relmada, Reviva, Rovi, Sage, Saladax, Sanofi, Seqirus, SK Life Science, Sumitomo Pharma America, Sunovion, Sun Pharma, Supernus, Tabuk, Takeda, Teva Pharmaceuticals, Terran, Tolmar, Vertex, Viatris y Xenon Pharmaceuticals. Ha prestado testimonio pericial para Janssen, Lundbeck y Otsuka, y ha formado parte de las Juntas de Monitoreo de Seguridad de Datos de Compass Pathways, IntraCellular Therapies, Relmada, Reviva, Rovi y Teva Pharmaceuticals. El Dr. Correll también ha recibido subvenciones de Boehringer-Ingelheim, Janssen y Takeda Pharmaceuticals, y ha recibido regalías de UpToDate. Es titular de opciones sobre acciones de Cardio Diagnostics, Kuleon Biosciences, LB Pharma, Medlink, Mindpax, Quantic y Terran.
-Prevalence, pre-existing conditions, and prior treatments among European adults diagnosed with tardive dyskinesia. https://www.sciencedirect.com/science/article/pii/S2772408524003211?via%3Dihub
-Conflictos de interés: Nayla Chaijale es empleada y accionista de Teva Pharmaceuticals. S. Reshef, Teva Branded Pharmaceutical Products R&D- Inc., Epidemiología, Economía y Resultados de la Salud Global, Parsippany, Estados Unidos. M. Forrest Gordon, Teva Branded Pharmaceutical Products R&D- Inc., Medicamentos Innovadores - Desarrollo Clínico Global, West Chester, Estados Unidos. A. Kurzeja, Teva Pharmaceuticals Europe B.V., Asuntos Médicos de la UE, Ámsterdam, Países Bajos, T. D. Maurice, Teva Pharmaceuticals Europe B.V., Investigación de Economía y Resultados de la Salud Global, Ámsterdam, Países Bajos.
REFERENCIAS
1.- Prevalence and Incidence of Huntington's Disease: An Updated Systematic Review and Meta‐Analysis. https://pmc.ncbi.nlm.nih.gov/articles/PMC10086981/
2.-Teva drafts NFL star Terrell Davis for tardive dyskinesia awareness drive https://www.fiercepharma.com/marketing/teva-drafts-nfl-star-terrell-davis-tardive-dyskinesia-awareness-drive
3.-Interview with Heather DeMyers See what Heather DeMyers has to say on Teva’s "Pivot to Growth" strategy and its impact on major products like AUSTEDO and AJOVY. https://www.newproductplanning.com/newproductplanningcom/exclusive-interview-heather-demyers-teva
4.-Tardive Dyskinesia - Epidemiology Forecast to 2032. https://pdf.marketpublishers.com/delveinsight/tardive-dyskinesia-epidemiology-insights-to-2025.pdf
5.-Cascadas terapéuticas y reacciones adversas a medicamentos. https://www.euskadi.eus/contenidos/informacion/uso_responsable_medicamentos/es_def/adjuntos/cascadas-terapeuticas.pdf
6.-Finally, Effective Treatments for Tardive Dyskinesia. https://www.thecarlatreport.com/articles/3453-finally-effective-treatments-for-tardive-dyskinesia
7.-Depression and suicidality with VMAT2 inhibitors in tardive dyskinesia A signal detection from the FDA Adverse Events Reporting System.https://onlinelibrary.wiley.com/doi/10.1002/pcn5.79
8.-Unique and overlapping mechanisms of valbenazine, deutetrabenazine, and vitamin E for tardive dyskinesia.https://www.nature.com/articles/s41537-025-00618-w
9.-Austedo. https://www.ema.europa.eu/en/medicines/human/EPAR/austedo
10.-¿Cuál es la diferencia entre deutetrabenazina y tetrabenazina? https://drugslib.com/medical-q-a/what039s-the-difference-between-deutetrabenazine-and-tetrabenazine-330/es/#gsc.tab=0
11.-Teva Third quarter 2025 Teva Pharmaceutical Industries Ltd. November 5, 2025 https://s24.q4cdn.com/720828402/files/doc_financials/2025/q3/Q325-Earnings-Presentation.pdf
12.-Do you recognize the magnitude of tardive dyskinesia (TD) impact? https://www.magnitude-of-td.com/
13.-TouchDown. You know this TD moves. https://www.theothertd.com/
14.-Teva lanza la campaña “The Other TD” para crear conciencia sobre la discinesia tardía con el apoyo del miembro del Salón de la Fama del Fútbol Americano Terrell Davis. https://nuevaprensa.web.ve/teva-lanza-la-campana-the-other-td-para-crear-conciencia-sobre-la-discinesia-tardia-con-el-apoyo-del-miembro-del-salon-de-la-fama-del-futbol-americano-terrell-davis/
15.-Cost-effectiveness of valbenazine compared with deutetrabenazine for the treatment of tardive dyskinesia. https://www.tandfonline.com/doi/full/10.1080/13696998.2020.1867443#abstract Crítica: https://www.tandfonline.com/doi/full/10.1080/13696998.2021.1948230 Respuesta: https://www.tandfonline.com/doi/full/10.1080/13696998.2021.1948233
16.-VMAT2 inhibitors for the treatment of tardive dyskinesia: a narrative review.https://www.cambridge.org/core/journals/cns-spectrums/article/vmat2-inhibitors-for-the-treatment-of-tardive-dyskinesia-a-narrative-review/76877F677766141404FC42B8030D9C51#article
17.-Healy D, Le Noury J, Harris M, et al. Mortality in schizophrenia and related psychoses: data from two cohorts, 1875–1924 and 1994–2010. BMJ Open 2012;2:e001810. doi:10.1136/bmjopen-2012- 001810
18.--Lessons from the RADAR trial. https://joannamoncrieff.com/2023/10/02/lessons-from-the-radar-trial/
19.- Early Dose Reduction or Discontinuation vs Maintenance Antipsychotics After First Psychotic Episode RemissionA Randomized Clinical Trial. https://jamanetwork.com/journals/jamapsychiatry/fullarticle/2839607
20.- Commentary: Does First Year Treatment With an Antipsychotic Lead to Long-Term Harm? https://www.madinamerica.com/2025/11/commentary-does-first-year-treatment-with-an-antipsychotic-lead-to-long-term-harm/
21.- Antipsicóticos como contención farmacológica en residencias geriátricas: desde el despropósito legal hasta la ética necesaria. https://accesojustomedicamento.org/antipsicoticos-como-contencion-farmacologica-en-residencias-geriatricas-desde-el-desproposito-legal-hasta-la-etica-necesaria/

Fergie Chambers facing US extradition from Spain. Fergie Chambers, detenido en Ibiza para extraditarlo a Estados Unidos. ENG ESP
The use of counterterrorism powers to target left-wing activists and political movements. Uso de legislación contraterrorista para lesionar actividades propalestina.
Publicado hace 3 días.
Ética médica. Están torturando hasta matar a nuestro compañero Abu Safiya. ¿Qué vas a hacer?
¿Vas a permanecer en silencio e impasible?
Publicado hace 6 días.
España. Evacuaciones sanitarias sanitarias infantiles. No hay motivo para el orgullo, señora ministra
Le pedimos un esfuerzo mayor para evacuar a más pacientes palestinos.
Publicado hace 11 días.
Dr Abu Safiya. "Esta es la última vez que me ves". "This is the last time you'll see me" ESP ENG
Physicians for Human Rights Israel, (PHRI): riesgo «inminente» para la vida del doctor Hussam Abu Safiya. Physicians for Human Rights Israel of an "imminent" risk to the life of Dr. Hussam Abu Safiya
Publicado hace 13 días.
Israel. The physician: “I didn’t come to treat you. I came to torture you.” El médico: «No vine a curarte. Vine a torturarte».
Tortures unrelated to interrogations or intelligence gathering. Torturas no relacionadas con interrogatorios ni con la recopilación de información
Publicado el 30 de junio.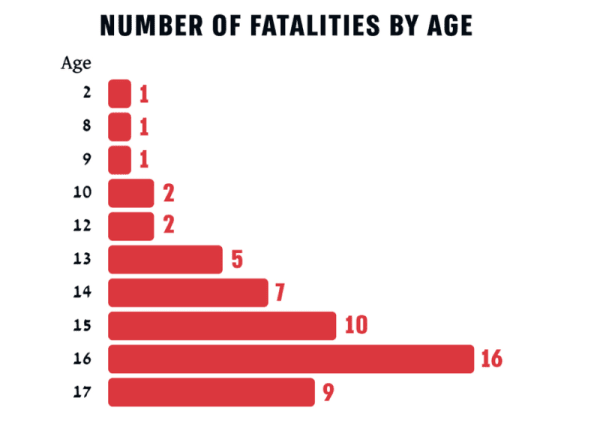
Unshielded Childhood: 54 Palestinian children and teenagers killed by Israel in the West Bank in 2025. Infancia inerme. 54 niños-adolescentes asesinados en 2025 en Cisjordania. ENG ESP
As of 6 June 2026, Israel was still holding 18 of the 54 bodies. A 6 de junio de 2026, Israel mantiene secuestrados 18 de los 54 cuerpos.
Publicado el 29 de junio.
British Medical Association votes down IHRA anti-semitism definition. La Asociación Médica Británica rechaza la definición de antisemitismo de la IHRA. ENG ESP
To protect doctors criticizing Israel from NHS discipline. Para proteger a los médicos que critican a Israel de posibles sanciones en el Servicio Nacional de Salud.
Publicado el 28 de junio.
The Israeli Medical Association (IMA) is acting like the Israel Defense Forces (IDF)'s mouthpiece. La Asociación Médica Israelí (AMI) actúa como portavoz de las Fuerzas de Defensa de Israel (FDI). ENG ESP
"How can we, doctors, stand aside?". "¿Cómo podemos nosotros, los médicos, quedarnos al margen?"
Publicado el 27 de junio.Ver más / See more
